longer summary:
(intro)
- covid has really put a spotlight on masks and their efficacy
- guidelines from various health agencies have been inconsistent
- "widespread disinformation and politicization of masks" isn't helpful
- masks & respirators block exhaled particles from those infected
(methods)
- the authors searched related terms and collected as many english-language studies related to face masks, respirators, covid, the flu, and contagious viruses as they could.
- they sifted through them and found 29 trustworthy "high evidence" experiments (all randomized controlled trials - RCTs). (those are all listed here)
- they also looked at mask guidelines from the WHO, CDC, UK Health Security agency, the Australian New Zealand Clinical Trials Registry, and the US National Institutes of Health trial registry. (search terms here)
(previous meta-analyses on masks and respirator use)
- a lot of the existing studies don't agree on how helpful masks are!
- it is hard to compare them because they all use slightly different methods and measure results differently
(use of masks and respirators in healthcare settings)
(RCTs in healthcare settings)
- they found 7 studies comparing regular masks with respirators (N95 or better) when used by healthcare professionals in hospitals, clinics, doctor's offices, etc.
- 6 of them were conducted pre-covid! only 1 of these is post-2020 recent.
- a "key design issue" is whether the healthcare workers studied wore their respirators all day long, or if they took them off some of the time.
- intermittent mask use in a hospital is not protective.
- n95 respirators have been repeatedly proven to be more effective than medical/surgical masks for a number of respiratory infections.
- ventilation systems mix and disperse air within the building
- why would you only need a mask in "close contact" or "aerosol generating procedures"? doesn't make much sense in light of this evidence
- ventilation systems in many buildings are designed for climate control, not air quality or infection prevention
- respiratory aerosols can be dispersed to different rooms & accumulate throughout the building
- one pre-covid study compared cloth masks & medical masks
-- flu-like illness was higher in those with cloth masks
-- no significant difference in lab-confirmed infections
-- a 2020 review of this study found that cloth masks washed in a washing machine (60 c or 140 f) are as effective as medical masks
(Observational, case-control, cohort, and experimental studies in healthcare settings)
- lots of non-randomized (not RCT) studies over the past 50 years
- these have studied SARS, tuberculosis, respiratory syncytial virus, and pertussis (whooping cough)
- another meta analysis from 2020 looked at SARS, Middle East respiratory syndrome (MERS), and early covid data
-- showed 85% protection with medical masks & respirators (analyzed together)
-- greater protection attributed to higher n95 use
- respirators are recommended for tuberculosis but there are no studies proving that they are effective in a clinical setting
- one laboratory study found lower airborne transmission of tuberculosis with a medical mask
- another found that medical masks help protect hospital patients from contracting pertussis
- real-world studies find that there is some protection with cloth masks, more protection with medical masks, and the most protection with respirators.
- lab studies show low filtration from surgical masks compared to n95s
- protection improves with more layers in the mask
- N95s have 8-12x greater protection than surgical masks
- 2 or more surgical masks increase protection, but still not as much as an N95.
(use of masks in community for primary prevention)
(RCTs in community settings)
- they reviewed 12 RCTs researching facemasks in community settings (with the goal of protected uninfected mask wearers)
- some showed protective effect of masks, but others didn't
- low rates of mask-wearing in many cases makes it harder to measure
- the biggest well-designed RCT showed "statistically significant protection" against symptomatic covid infections
- masks are protective in epidemics, especially if widespread mask-wearing begins early and people wash their hands sufficiently
- another recent meta-analysis found that mask use combined with hand hygiene protected against flu-like and covid-like illnesses, as well as lab-confirmed flu infections
- a recent randomized trial in Norway found 29% protection with surgical masks vs. no mask at all
(observational, case-control, cohort, and laboratory studies in community settings)
- observational studies aren't always reliable because extra factors aren't controlled for, so take these with a grain of salt
- cloth masks were shown to be effective during the 1918 flu outbreak
- in 2002-03, masks were found to be effective against SARS infection in china, hong kong, and canada, where mask usage was high
- several studies find masks to be protective in high-risk situations
- outside of senior care & long term care facilities, the highest risk community setting is AT HOME.
-- close, prolonged exposure at home
-- use of masks at home reduced risk of infection by 79% when worn before the infected household member showed symptoms. <-- **PREsymptomatic transmission**
- one "well designed" study conducted during covid showed that consistent mask use in indoor public settings reliably reduced risk of infection
-- 83% protection from N95s
-- 66% protection from surgical mask
-- 56% protection from cloth mask
- numerous models demonstrate reduced population transmission with mask use
(children)
- couldn't find any randomized control trials
- a japanese study in 2014-2015 found masks protective against flu transmission amongst schoolchildren, especially in older age groups (9-12 years old)
- another study showed a "surge" of covid infections when school mask mandates were listed
- covid outbreaks were 3.5 times more likely in schools without a mask mandate, in a study in arizona
- other studies have mixed results: children don't wear masks as reliably, parents and teachers might be concerned about "impact on speech, language and learning," parents may be anxious about children wearing masks, and smaller child-sized masks may be harder to find
- in august 2020, the WHO and Unicef recommended masks for children aged 5-18, and said that cloth masks should be worn if physical distancing isn't an option
- the CDC recommended universal mask use in all schools grades K-12
- during a mandatory masking period, one infected teacher removed their mask to read to the class, "resulting in a large outbreak, despite spacing of 6 ft between desks"
(mask use as source control)
source control: "mask use by a person with an infection to protect others"
- infected people breathe out "large amounts" of infected particles
- "long range airborne transmission" of covid has happened at church events, choir practices, and on planes
(randomized controlled trials)
- 4 studies about mask wearing as source control
- first trial found no difference between surgical masks vs no mask, but the study ended early because it didn't have many participants and was interrupted by the 2009 flu pandemic
- a study of hajj pilgrims found lower rates of flu-like illness when the infected wore masks. but there wasn't much reliable mask-wearing, and lab reports of infection were not significantly different
- a third RCT: 245 patients who visited a fever clinic
-- no difference between the two groups themselves, but the households of mask-wearers had lower rates of infection
- another study measured the amount of flu and covid viruses exhaled by infected patients with & without masks
-- significant reduction in exhaled aerosols in both groups
-- notable amount of virus found in aerosols (vs large droplets)
(other source control studies)
- the amount of flu virus coughed onto a petri dish was reduced when the patient was wearing a mask/respirator
- N95s and medical masks prevented any measurable particles, but seven non-masked patients coughed enough to test positive
- a flu study found a "threefold reduction of viral particles" with the use of medical masks
- aerosols had 9 times as much virus than larger exhaled particles did
- conclusion: flu is an airborne virus
- another study: all face coverings reduce exhaled covid virus. N95s were best, even without training or fit-testing.
- evidence that tuberculosis transmission is reduced with mask wearing by those infected
- there aren't a lot of good trials, but masks are still recommended for tuberculosis by the WHO, CDC, and European Centre for Disease Prevention and Control
(selection of masks or respirators)
(occupational health and safety factors)
- most occupational hazards are addressed by removing the hazard or removing the worker from the unsafe situation
- unfortunately, you can't remove healthcare workers from hospitals
- the importance of respirators in this situation "has never been explicitly recognized"
- traditional infection control measures only consider how the virus is transmitted
- a risk-based approach might be better, to take into consideration "the pathogen, the setting, the occupational health and safety requirements, availability of treatment or vaccines, and uncertainty"
- availability of masks is one of the most important factors
- organizations should make sure to have enough respirators on hand for front line workers
- mask wearing rates are affected by perceived risk
- studies during lower risk periods might show different rates
(fit testing of respirators)
- for maximum protection, a respirator should fit snugly against your face with no gaps
- different face shapes may require different mask types (dome vs duckbill shape, head straps vs ear loops)
- ear loop masks do not fit as well
- a well-fitting respirator may restrict breathing, especially for those with asthma, COPD, or similar
- carbon dioxide can build up in the mask, but does not usually exceed occupational safety limits
- if you have breathing difficulties, talk to your doctor about mask & protection options
(mask mandates, universal masking, and situational considerations)
- mask policies can vary quite widely and guidelines can change - sometimes it is recommended that only infected people mask; in other cases healthy people are also encouraged to mask
- an important factor is asymptomatic or presymptomatic transmission
- we've known for a long time that the flu can be transmitted asymptomatically
- covid has an even higher rate
- 30-50% of covid infections came from someone who had no symptoms
- people do not necessarily know they are infected! which supports the recommendation that everyone, symptoms or not, should wear a mask
- hospital-transmitted infections are a huge problem, and often deadly
- healthcare facilities that required masking for all staff had lower rates of infection than those that didn't
- risk of catching the flu in a hospital is reduced by 50% with mask mandates
- covid has really taught us a lot about disease transmission from those with no symptoms: supports universal masking during epidemics
(non-standardized practices around mask use during epidemics or pandemics)
- PPE shortages can happen during pandemics when demand suddenly spikes
- non-standard practices may need to be used:
-- wearing masks longer than usually recommended
-- reusing masks & respirators
-- double masking
-- using cloth masks in healthcare settings
- knotting ear loops to tighten & double masking may improve fit (better seal around the mask edges)
- a 3-ply cloth mask over a 3-ply medical mask resulted in an 85% reduction in particles emitted
(extended use and reuse of masks and respirators)
- if there aren't enough masks to go around, reusing masks makes more sense than wearing nothing at all
- there aren't really any guidelines on reusing masks, or wearing them longer than recommended
- extra germs on the outside of the mask might contaminate you more easily
- frequent hand-washing is recommended if you are going to be wearing a mask for a long time
- wearing masks for a long time might make them fit less well (less seal against the face)
- one study found bad seals in 38% of masks after they were worn for one shift (in healthcare); after five shifts, 93% failed the fit test
- most disinfection methods (soap, bleach, peroxide, UV light, heating) just damage the mask and reduce its effectiveness
- vaporized peroxide and UV irradiation seem to be the most effective
(use of cloth masks)
- when disposable masks were hard to find early in the pandemic, researchers started investigating ways to make cloth masks more effective
- cloth masks often weren't taken into account because planners assumed there would be enough medical masks & respirators available
- other homemade face coverings like neck gaiters, bandanas, and scarves have some protection, but not as much as medical masks or respirators
- one RCT found poor effectiveness in cloth masks
- cloth masks may actually be harmful if they are not washed in hot water daily
- cloth masks washed in a washing machine at a high temperature can be as protective as surgical masks
- poorly washed masks are not effective
- the authors do not recommend cloth masks in healthcare settings
- cloth masks may be helpful in community settings when higher quality masks are unavailable
(emerging areas in mask design)
ways masks can be improved: - better fit against the face (a good seal is important!)
- more tightly sealed medical masks
- make masks easier to take on and off (handling a dirty mask can get pathogens on your hands)
- test new fabrics that may be better at filtering air
- there are lots of new designs, but most have not actually been tested
(guidelines)
- currently, most guidelines assume infected droplets are either droplets or airborne
- it's actually more of a spectrum
- large and small droplets of various sizes were thought to only travel 1-2 meters at most
- it can actually be as far as 8 meters
- droplets are infectious at a much further distance than was previously thought
- only wearing a mask in close proximity to an infected patient does not sufficiently protect anyone
- it was previously thought the flu was only infectious through droplets, but it can stay airborne for long periods too
- in 2024 the WHO began recognizing droplets & aerosols as a continuum of respiratory particle sizes
- respirators/N95s are designed to protect against all of these
(summary of evidence and recommendations)
` - controversy around masks is not new
- happened in 2003 with SARS, 2009 with the flu, and in 2014 with ebola
- the final conclusion from all these studies? masks & respirators protect against respiratory infections
- respirators/N95s are better than surgical/medical masks or KN95s or cloth masks
- any protection is better than none!
- it's not "droplet vs airborne" but rather a spectrum of infectious particle size
- "protection increases from cloth masks to surgical masks to N95 respirators"
- masks are more effective if worn by more people
- masks are more effective if people start wearing them early in an epidemic
- hand-washing must be emphasized so that you don't contaminate the mask or vice versa
- (one study showed masks were ONLY protective when wearers also washed their hands well and frequently)
- people are more likely to wear masks if they feel their risk is higher
- studies conducted during low-risk periods may not reflect mask-wearing rates during more severe outbreaks
- there is a disproportionate focus on masks as "source control" (only for people with symptoms)
-- many of these viruses are contagious before the infected person shows symptoms: presymptomatic & asymptomatic transmission
-- masks must be worn by those without symptoms during outbreaks in order to be effective
-- in healthcare settings (hospitals, care homes, etc), universal masking is the best bet to keep everyone safe
-- early widespread masking can "flatten the curve" better than only people with symptoms wearing masks
- the "dramatic decline" of other contagious illnesses in 2020 is a great example of how non-symptomatic masking can preemptively reduce the spread of infection
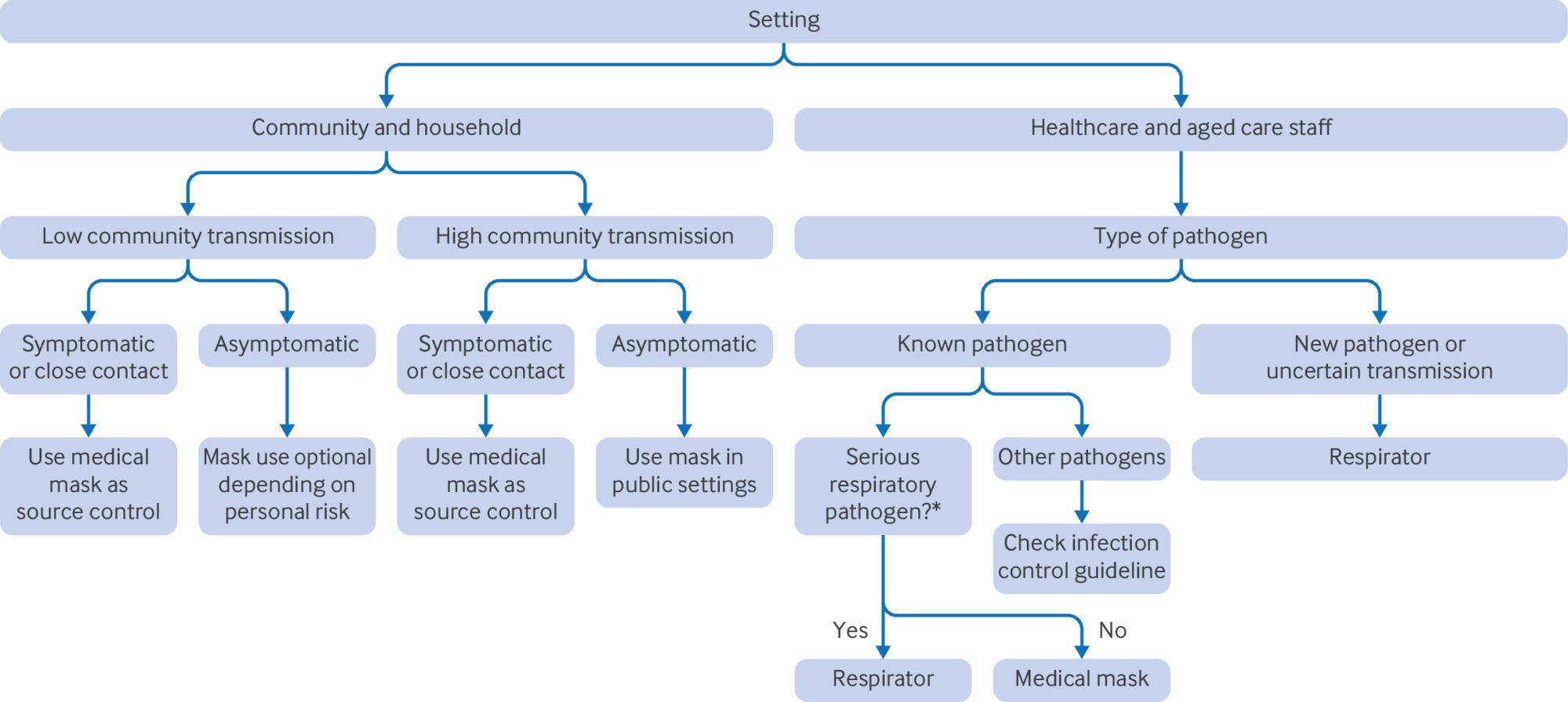
- mask policies are often broad and unchanging - it makes more sense to consider the specifics of each infection: -- how does it spread between people? -- does it have a lot of asymptomatic transmission? -- who does it infect? -- what is the environment like? - mask policies work best when tailored to the targeted situation
- rising waves of infection (like covid has regularly) are a good time for everyone to wear a mask
- levels of masking can change to reflect infection rates in the community:
1. earlier masking in high-risk settings like hospitals & other healthcare (start earlier and continue longer)
2. more widespread masking in public transport & crowded public spaces
3. community-wide mask mandates only as a last resort if the previous steps do not contain the infection
- protecting healthcare workers is the highest priority
- high risk settings like hospitals & care homes should have flexible plans for when & where to require masking
- preventing hospital-acquired infections is also an important goal
- hospitals should require masking at much lower rates of illness transmission to protect patients and workers
- research needs to be done to further protect workers who treat patients with infectious illnesses
- respirators should be prioritized:
-- when the disease is severe and has a high rate of deaths
-- when healthcare worker absenteeism will impact functioning of a hospital/health setting
-- when there is no vaccine or treatment available
- in an outbreak, changes like improved ventilation may not happen fast enough, so masks are an important protection
- masks should be used as a precaution - there was a "large, fatal outbreak" of SARS in toronto when workers refused to wear masks
- by contrast, healthcare workers in vancouver wore respirators that were provided, and did not have an outbreak
- this has been reflected in the covid pandemic, where disagreements about masking led to many healthcare workers dying due to poor masking rates
- evidence supports constant, continuous masking (not occasional) to reduce the spread of infection
- there needs to be a "major paradigm shift" with mask guidelines in order to adequately protect both workers and patients
- only using masks in "high risk" situations can save money, but... it doesn't really work, and ultimately costs more in the long run
who should wear masks, and when? decision tree:
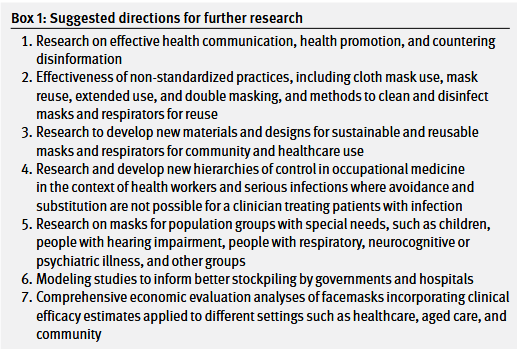
(research gaps and the way forward)
- more research is needed to fill in knowledge gaps
{kind=link}
- more sustainable and reusable products to avoid shortages
- clear guidelines on mask use, reuse, disinfection
- investigate "non-standard" methods like cloth mask use and double masking
- cost effectivity of stockpiling masks and other PPE (shortages occur during every pandemic)
- stockpiling was insufficient for covid-19 and the 2009 flu pandemic
- cost effectiveness of supplying masks for all workers to reduce hospital-inquired infections and deaths of patients
- strategies to improve rates of mask-wearing
- people are more likely to wear masks when they think their risk is high, but this is a case where early proactive mask-wearing by asymptomatic people will make a huge change in the scale of an outbreak
- improve community engagement: -- work with people who can't just wear a mask (kids, people with asthma or COPD, the elderly) to find other options to keep them safe
-- counter disinformation and politicization
-- improve people's understanding of current evidence and resulting guidelines
- contradictory policies early in the covid pandemic eroded public trust
- health leaders cannot hesitate or show uncertainty
- widespread disinformation and masks as "a stigmatizing political signal rather than a simple public health measure" demonstrate a need for further research on health communication and countering disinformation.
(limitations of review)
- randomized controlled trials are hard:
-- unpredictable rates of infection spread
-- people refusing to wear masks
-- how to measure follow-ups & how complex to make them
-- how to track very rare outcomes
-- no control group of non-masked people because this is unethical
-- many studies compare results in different ways: household vs healthcare, continuous vs intermittent mask use: tough to compare these in one review
-- they were only able to review english-language studies, so might have missed some
(conclusion)
- "there is ample evidence on the effectiveness of masks and respirators in community and healthcare settings."
- n95s/respirators are better than other masks and should be the first choice
- mask use is effecttive during high risk or high transmission periods, especially when worn by people with no symptoms
- "strong leadership is required to overcome politicization and polarization around masks"
- it's important to stockpile supplies & decide on guidelines ahead of time